Jho Institute for Minimally Invasive Neurosurgery Department of Neuroendoscopy
Home | About Dr. Jho | Overview | Table of contents | Patient Registration Form | Directions, Contact & Hotel Information
Spine Diseases
Brain Diseases
Glossopharyngeal Neuralgia: Dr. Jho's Endoscopic MVD Surgery, Minimally Invasive Glossopharyngeal Nerve surgery
Dr. Jho's Microvascular Decompression of the Glossopharyngeal Nerve
Professor & Chair, Department of Neuroendoscopy
Jho Institute for Minimally Invasive Neurosurgery
After working for approximately 20 years with Professor Jannetta (who pioneered the development of various Jannetta procedures for microvascular decompression), Dr. Jho developed minimally invasive endoscopic microvascular decompression surgery. Microvascular decompression surgery was originally pioneered by Professor Jannetta, who has spent his lifetime in a neurosurgery career exploring various neurovascular compression syndromes.
Microvascular decompression is a surgical treatment for cranial nerve disorders such as trigeminal neuralgia, hemifacial spasm, vertigo, tinnitus, glossopharyngeal neuralgia, and spasmodic torticollis. Microvascular decompression (which consists of placement of small synthetic sponges between the compressing blood vessels and the affected cranial nerves) carries a good chance of relieving the symptoms associated with these disorders.
Discussion
When blood vessels cross and compress cranial nerves, various characteristic symptoms develop depending upon which cranial nerves are compressed. Trigeminal neuralgia develops by blood vessel compression of the trigeminal nerve, hemifacial spasm by compression of the facial nerve, intractable positional vertigo by compression of the vestibular nerve, tinnitus by compression of the cochlear nerve, glossopharyngeal neuralgia by compression on the glossopharyngeal nerve, and spasmodic torticollis by pressure on the spinal accessory nerve and upper cervical nerves. Cranial nerve surgery is done through a small skull opening behind the ear and is referred to as retromastoid craniectomy. Skin incisions are usually only two inches in length.
A: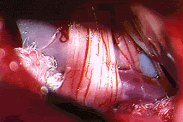 B:
B:
B:Figure 1. An arterial loop (PICA) is progressively decompressed with Teflon placement in a patient with glossopharyngeal neuralgia (A). Teflon placement can be seen at the completion of microvascular decompression of the ninth and tenth cranial nerves (B).
Practice Manager: Robin A. Coret
Tel : (412) 359-6110
Fax : (412) 359-8339
Address : JHO Institute for Minimally Invasive Neurosurgery
Department of Neuroendoscopy
Sixth Floor, South Tower
Allegheny General Hospital
320 East North Avenue
Pittsburgh, PA 15212-4772


Copyright 2002-2032