Jho Institute for Minimally Invasive Neurosurgery Department of Neuroendoscopy
Spine Diseases
Brain Diseases
Acoustic Neuroma, Acoustic Tumor: Dr. Jho's Hearing-Preserving Acoustic Neuroma Surgery
Dr. Jho's Minimally Invasive Retrosigmoid Approach Acoustic Neuroma Surgery
Professor & Chair, Department of Neuroendoscopy
Jho Institute for Minimally Invasive Neurosurgery
Dr. Jho's acoustic tumor surgery
Dr. Jho prefers a retromastoid or retrosigmoid approach for acoustic tumor surgery because it results in high probability of the preservation of the facial nerve and hearing nerve functions. A retromastoid approach is made with an approximately one-inch (or three-cm) skull opening via a two-inch (or five-cm) skin incision behind the ear. Metallic brain retractors that are used by other surgeons for routine brain surgery are never used (in order to avoid any unwanted retraction injury to the brain). Hearing and facial nerve functions are continually monitored electrophysiologically throughout the operation. The operating microscope and an endoscope are used for surgical visualization. The tumor is excised with delicate microdissection. The skull opening is reconstructed and the incision is closed cosmetically. A small bandage is applied.
A: 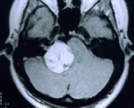 B:
B: 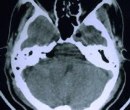
B: Figure 1. A preoperative MR scan, axial view (A), reveals an acoustic tumor. An immediately postoperative axial CT scan (B) demonstrates complete removal of the acoustic tumor accomplished via a retromastoid craniectomy approach.
A:  B:
B: 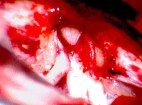
B: Figure 2. An intraoperative photograph shows tumor removal at the internal auditory canal during a retromastoid craniectomy approach (A). This intraoperative photograph demonstrates complete removal of an acoustic neuroma and the preserved facial and hearing nerves (B).
A:  B:
B: 
B: Figure 3. Immediate postoperative patient photographs demonstrate normal facial nerve function following retromastoid craniectomy for acoustic tumor removal. The patient's hearing was also well preserved.
Overview
Acoustic neuromas are benign brain tumors usually arising from the vestibular nerve (balance nerve), most commonly from the superior vestibular nerve. Sound travels through the ear drum to the middle ear and enters into the inner ear organ. Sound is converted to nerve impulses, and the nerve impulses travel through the hearing nerve (cochlear nerve) to the brain. The inner ear organ has a balance organ in addition to a hearing organ. This balance organ system is extended to the brain via two nerve cables named the superior vestibular nerve and inferior vestibular nerve. The facial nerve also travels together towards the brain.
The cochlear nerve, the two vestibular nerves (superior and inferior), and facial nerve travel together in the inner ear canal to enter into the brain. When an acoustic tumor develops, it most often develops at the superior vestibular nerve in the inner ear canal (internal acoustic canal). Thus, the tumor compresses the hearing nerve (cochlear nerve) causing tinnitus and hearing impairment. It can also cause dizziness or vertigo by balance nerve dysfunction. The facial nerve tolerates compression better than the other nerves so that facial weakness develops very late. If facial nerve weakness develops earlier than hearing loss due to a tumor, it is more likely that the tumor is a facial nerve neuroma (which is rare).
Although hearing tests are required for hearing evaluation in aiding the diagnosis, definitive diagnosis of an acoustic neuroma is made with MR scans of the brain. Treatments for acoustic neuromas consist of observation with interval MR scans, surgical removal, or radiosurgery. Large tumors generally require surgical removal, while small tumors also have the option of radiosurgery treatment. Microsurgical removal of a small tumor can achieve a 90-99% chance of normal facial function and a 60-80% chance of hearing preservation postoperatively. Large tumors carry higher chances of temporary facial weakness and hearing loss postoperatively.
In order to avoid serious complications such as brain injury, brain retractors are not used at all in the Jho Institute for Minimally Invasive Neurosurgery. For removal of small tumors, a two-inch skin incision and a one-inch bone opening are carried out behind the ear. A tumor is removed under the operating microscope or an endoscope. A patient wears a small Band-Aid over the incision overnight. Hospital stay will be two to three nights. For removal of a large tumor, a slightly larger incision may be required.
Practice Manager: Robin A. Coret
Tel : (412) 359-6110
Fax : (412) 359-8339
Address : JHO Institute for Minimally Invasive Neurosurgery
Department of Neuroendoscopy
Sixth Floor, South Tower
Allegheny General Hospital
320 East North Avenue
Pittsburgh, PA 15212-4772


Copyright 2002-2032
