Jho Institute for Minimally Invasive Neurosurgery Department of Neuroendoscopy
Spine Diseases
Brain Diseases
Thoracic Disc Surgery: Dr. Jho's Endoscopic Thoracic Disc Herniation Surgery
Dr. Jho's Minimally Invasive Thoracic Disc Surgery: Endoscopic Transpedicular Thoracic Discectomy
Professor & Chair, Department of Neuroendoscopy
Jho Institute for Minimally Invasive Neurosurgery
Current conventional thoracic disc surgery involves either an extensive open chest approach or radical extensive posterior approaches. In order to make a thoracic disc operation as minimally invasive as a cervical or lumbar disc operation, endoscopic transpedicular discectomy was developed by Dr. Jho. Obtaining surgical access to the thoracic spine with minimal anatomic disruption has generally been more difficult than obtaining minimally invasive access to the cervical or lumbar spine. The Jho procedure for Thoracic Disc Herniation involves a two-cm skin incision at the posterior thoracic area, insertion of a 1.5-cm-diameter trocar, and removal of the protruded disc under endoscopic guidance (Figure 1). Only an overnight hospital stay is required since postoperative discomfort is relatively minimal. He also uses an alternative minimally invasive method with an endoscopic transthoracic approach when surgical access to the frontal aspect of the spinal cord is necessary.
A: B:
B:
B:Figure 1. Schematic drawings demonstrate removal of the protruded disc under 70-degree endoscopic visualization (A, B). C: the spinal cord, D: the protruded disc.
The incidence of thoracic disc herniation is low compared to that of cervical or lumbar disc herniation, likely due to the unique anatomy and function of the thoracic spine. Although a soft disc herniation is possible in the thoracic spine, most thoracic disc herniation is due to a calcium-containing hard disc protrusion. This can occur spontaneously or after an injury. Clinical symptoms are produced by: (1, axial pain) local compression of the surrounding anatomy causing thoracic back pain; (2, radiculopathy) compression of the passing nerve root causing radiating pain along the rib cage, chest, and abdomen; or (3, myelopathy) by compression of the spinal cord causing numbness in the legs, difficulty in walking, and disorders in bowel and/or bladder control.
Conventional surgery for thoracic disc herniation consists of an extensive open-chest operation (transthoracic anterior discectomy) or various types of extensive posterior operations. A less invasive procedure was recently developed elsewhere, called an endoscopic transthoracic discectomy. However, this procedure is still rather invasive. Three to four skin incisions are still required at the chest wall, and chest tube drainage is often required postoperatively. Dr. Jho uses endoscopic transthoracic techniques in selective cases when the frontal aspect of the spinal cord has to be approached directly.
In order to make surgery for thoracic disc herniation truly less invasive, Dr. Jho has developed endoscopic surgery through a transpedicular approach. The operation involves a small incision at the posterior thoracic area, insertion of a small trocar towards the herniated disc and removal of the herniated disc under an endoscope. The surgical approach is made under the guidance of a 0-degree-lens endoscope. Then, the protruded disc in front of the spinal cord is removed under a 70-degree-lens endoscope. A 70-degree-lens endoscope directly visualizes the herniated disc located anteriorly to the spinal cord, as a rear-view-mirror in a car does. When surgery is finished, a small bandage is placed at the incision site. Surgery has been performed on an outpatient or overnight stay basis.
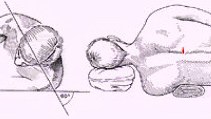
Figure 2. Schematic drawings demonstrate a patient's positioning, and the line of a skin incision that is approximately two cm in length.
A: B:
B: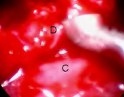 C:
C: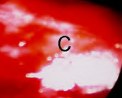
B: C:Figure 3. Sequential intraoperative endoscopic images ((A,B,C) demonstrate disc removal. C: the spinal cord, D: the protruded disc. Herniated calcified disc compressing the spinal cord is exposed (A). With a specially designed curet, herniated disc is separated and lifted from the spinal cord for removal (B). When the herniated disc is removed, the compressed spinal cord expands back to normal position (C).
A: 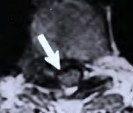 B:
B: 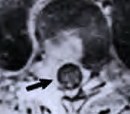
B: Figure 4. MR scans, axial views, depict a protruded disc preoperatively (A, arrow) and its complete removal postoperatively (B). The bright signal in the postoperative image represents the surgical trajectory. The spinal cord (the black circular structure) is well decompressed (B, arrow).
A:  B:
B: 
B: Figure 5. A preoperative MR scan, sagittal view (A), shows a herniated thoracic disc (arrow). The corresponding postoperative MR scan (B) demonstrates removal of the herniated portion of disc. The spinal cord is well decompressed (arrows).
Facts About This Surgery
Discussion
As mentioned previously, this minimally invasive procedure combines the transpedicular approach to thoracic discs with the technology of endoscopic surgery. Using the transpedicular approach provides the surgeon an alternative to the extensive posterolateral approach and to the thoracotomy approach (which is open chest surgery). The utilization of an endoscope, which improves visualization much like the periscope of a submarine or the rear-view mirror on an automobile, further enhances the transpedicular approach in accomplishing the goal of successful disc resection. This provides the patient with a better chance of having the symptoms of pain or leg weakness resolved. The use of an endoscope and a less invasive surgical approach also leads to decreased postoperative complications. This surgery is usually done on an outpatient or overnight basis.
Reference
Practice Manager: Robin A. Coret
Tel : (412) 359-6110
Fax : (412) 359-8339
Address : JHO Institute for Minimally Invasive Neurosurgery
Department of Neuroendoscopy
Sixth Floor, South Tower
Allegheny General Hospital
320 East North Avenue
Pittsburgh, PA 15212-4772


Copyright 2002-2032